Message from Kathy Hubble, CEO Amelio Health

Amelio Health Pain Program Details
Amelio Health is a digital therapeutic program that empowers participants with the knowledge to make informed choices about their recovery.
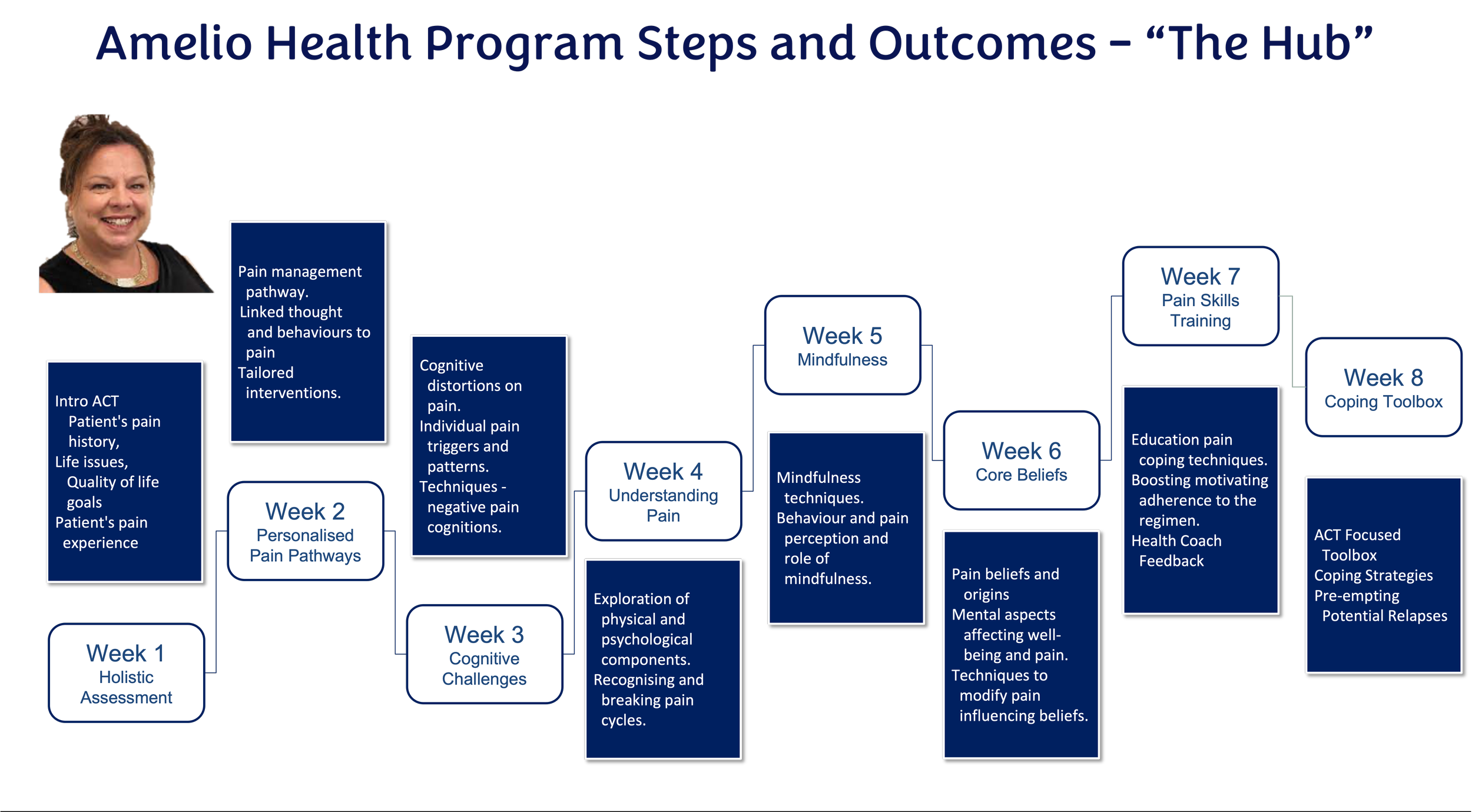
An eight-week intensive program, each module delivered in video format is embedded with core competencies from The International Association for the Study of Pain (IASP) and Bloom's Taxonomy of Learning Theory.
Data from biopsychosocial scores, wearables, and daily pain diaries is analysed and provided to live health coaches to drive behaviour change 24/7.
AI provides rules for closed-loop learning, predictive behaviour and decision support for Health Coaches, nudging at precise times for best outcomes.
AI provides automation of reporting to stakeholders. For the first time, data provides a 24/7 visual of how pain impacts a person's biopsychosocial life, and then AI drives precise nudging at the most opportune time.
“We have had people with chronic pain and opioid use disorders return to work after more than 5 years with a claim, releasing hundreds of thousands of dollars after doing the Amelio Health Program”
GIO Australia
“Our case managers have learned how to engage with people suffering with chronic pain and assist them to move forward after completing the Amelio Health Integrated Learning. This was essential in understanding the reported outcomes.”
RTW UK


Our aim is to make reducing the cost of complex claims simple for case managers.
What reporting is provided on people's progress, and on what basis?
The outcomes from the psychosocial tools, FitBit analysis, medication use, and learning modules are reported to case managers at weeks 2,4 and 8.
The data from Fitbits, psychosocial outcome scores, feedback from AH coaches, and pain diaries provide’s a 24/7 biopsychosocial visability of how pain is impacting a persons’ life.
AI predicts the best path to recovery for each individual based on their values and needs.
Weeks 5 - 8 are focused on increasing capacity and returning to work. This includes those that are employer-disconnected.
All reports are password-protected and sent direct to case manager’s email.



Fundamental Principles and Areas of Innovation
The program is exclusively online, so people in regional and remote areas can access it from their own homes. No need for costly flights and accommodation to attend a face-to-face program. This also reduces the risk of behaviour changes reversing on returning home.
AH focuses on Acceptance and Commitment Therapy and individuals engaging with their own data to see how the strategies they are learning has changed their pain.
Our early research highlighted the need for positive feedback mechanisms for long-lasting change. Bloom's learning theory, wearable bio data loggers, personal mobile applications, and health coaches are all elements of positive feedback and ongoing monitoring to foster an environment for sustainable change in health and lifestyle outcomes.
The remote online nature of the program is ideal for patient privacy and AH is fully HIPPA compliant.
Patients find by participating in the program, individuals can experience benefits such as
reduced stress,
improved mental clarity,
and better pain management.
Further Reading
1. Lewin, A. M., M. Fearnside, R. Kuru, B. P. Jonker, J. M. Naylor, M. Sheridan, and I. A. Harris. 2021.
“Rates, Costs, Return to Work and Reoperation Following Spinal Surgery in a Workers’ Compensation
Cohort in New South Wales, 2010-2018: A Cohort Study Using Administrative Data.” BMC Health Services
Research 21 (1): 955
2. Deloitte Australia Access Economics. 2019. “The Cost of Pain in Australia | Deloitte Australia | Deloitte
Access Economics, Healthcare, Public Sector.” Deloitte Australia. April 3, 2019.
3. Chu, Larry F., Martin S. Angst, and David Clark. 2008. “Opioid-Induced Hyperalgesia in Humans: Molecular
Mechanisms and Clinical Considerations.” The Clinical Journal of Pain 24 (6): 479–96.
4. Di Donato, Michael, Ting Xia, Ross Iles, Rachelle Buchbinder, and Alex Collie. 2021. “Patterns of Opioid
Dispensing and Associated Wage Replacement Duration in Workers with Accepted Claims for Low Back
Pain: A Retrospective Cohort Study.” Pain, November. https://doi.org/10.1097/j.pain.0000000000002539.
5. Williams, A. C., M. K. Nicholas, P. H. Richardson, C. E. Pither, D. M. Justins, J. H. Chamberlain, V. R.
Harding, J. A. Ralphs, S. C. Jones, and I. Dieudonné. 1993. “Evaluation of a Cognitive Behavioural Programme for Rehabilitating Patients with Chronic Pain.” The British Journal of General Practice: The Journal of the Royal College of General Practitioners 43 (377): 513–18.
7.Feliu-Soler A, Montesinos F, Gutiérrez-Martínez O, Scott W, McCracken LM, Luciano JV. Current status of acceptance and commitment therapy for chronic pain: a narrative review. J Pain Res. 2018 Oct 2;11:2145-2159. doi: 10.2147/JPR.S144631. PMID: 30323649; PMCID: PMC6174685.
8.Lance M McCracken, professor of clinical psychology1, Lin Yu, lecturer in psychology2, Kevin E Vowles, professor of clinical health psychology3 2022 “New generation psychological treatments in chronic pain” BMJ 2022;376:e057212
9.Tefera YG, Gray S, Nielsen S, Collie A. Preoperative opioid use and postoperative return to work following spinal surgery in workers' compensation settings: A systematic review and meta-analysis. Int J Surg. 2024 Jan 4. doi: 10.1097/JS9.0000000000001035. Epub ahead of print. PMID: 38181114.